Home
HomeThyroid Biopsy
Fine needle aspiration (FNA) biopsy of the thyroid nodule is the aspiration of thyroid cells using a very thin needle through the skin. It is an outpatient procedure performed in the office. The needle used is thinner than the one for drawing blood and is attached to a syringe to apply suction during the biopsy. It is a simple procedure, similar to drawing blood from your arm.
THYROID BIOPSY
- The biopsy is done under ultrasound guidance in our office.
- There will be a cytologist present in the room to prepare and evaluate the biopsy samples
- The average procedure time is approximately a few minutes
- We utilize local anesthesia with the spray to the skin and local injection of Lidocaine
- Ice pack is placed on the biopsy site for 10 min after the biopsy
- Patients usually experience little to no pain during the procedure.
- If the patient is on Fish Oil, Vitamin E, Coumadin, other blood thinners, or aspirin, it needs to be stopped for 5 days before the biopsy.
- Someone has to drive you in and out on the biopsy day.
- You do not need any preparation: no fasting, no restrictions after the biopsy.

Biopsy under ultrasound guidance

Ultrasound guidance

Slides preparation by cytologist
Follow up care for the patients AFTER THYROID BIOPSY
- You can apply an ice pack for 10-20 minutes two or three times if needed
- Tylenol may be used for pain.
- Call the office immediately if you develop neck edema (a swollen, large hematoma), difficulty breathing, fever, or chills. Our office number is 732-792-5003
- The result is available at your follow-up appointment in about 1 week
- Bring your imaging studies: a hard copy of the film or the CD disc with your ultrasound study
- It is recommended that you have a driver with you

Ultrasound view of the Thyroid Nodule in the right thyroid lobe
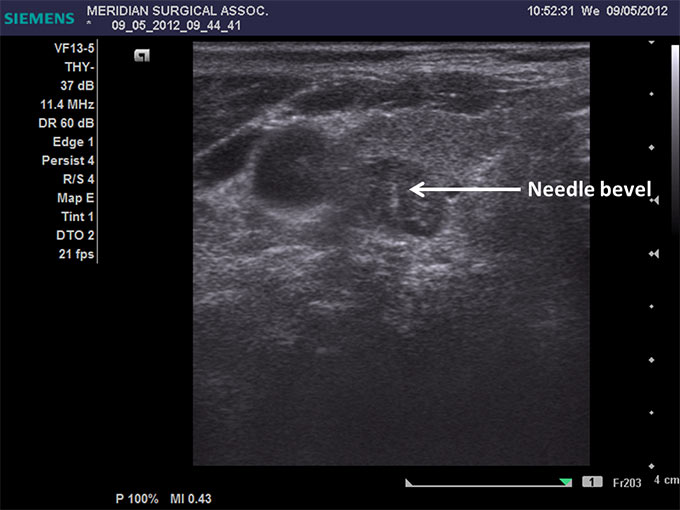
Ultrasound-guided fine needle aspiration (FNA) biopsy of the right thyroid nodule (needle bevel is indicated by arrow)
The Bethesda System for Reporting Thyroid Cytopathology with Risk of Malignancy.
Bethesda Category I. Nondiagnostic or Unsatisfactory (risk of malignancy 1-4%) - means that there are not enough or no cells present at all to make a diagnosis. This result would require additional testing and repeating the biopsy. If a biopsy of a solid nodule is non-diagnostic on three consecutive occasions, then surgery is indicated to rule out cancer.
Bethesda Category II. Benign (risk of malignancy 0-3%) - means that the nodule or lump is not a malignant tumor. Even though the biopsy is benign, there is still a small possibility of cancer because no technique is 100% accurate. If this is the reason, the patient still needs to follow up with an annual thyroid ultrasound to ensure there are no changes in the nodule's size or appearance.
*Bethesda Category III. Atypia of Undetermined Significance (AUS) or Follicular Lesion of Undetermined Significance (FLUS) (risk of malignancy 5-15%) - means that the result is inconclusive. However, there are some abnormal changes that were found, but not enough to make a diagnosis of cancer. Additional testing or surgery is required.
*Bethesda Category IV. Follicular Neoplasm or Suspicious for a Follicular Neoplasm (risk of malignancy 15-30%) - means that the result is inconclusive. However, there are significant changes present even compared to a prior Category III, but still not enough to make a diagnosis of cancer. Additional testing or surgery is required.
Bethesda Category V. Suspicious for Malignancy (risk of malignancy 60-75%) - there is a high likelihood of cancer, and surgery is indicated.
Bethesda Category VI. Malignant (risk of malignancy 97-99%) - means that the nodule is cancerous, and surgery is indicated.
[*- so-called indeterminate cytology]
(E.Cibas, AJCP, 2009)
Molecular Markers Assessment Genetic Analysis on THYROID FNA BIOPSY
Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer (RECOMMENDATION 8; THYROID, Volume 19, Number 11, 2009) considered use of molecular markers (e.g., BRAF, RAS, RET/PTC, Pax8/PPARg, or galectin-3) for patients with indeterminate cytology on FNA to help guide management (Recommendation rating: C). Guidelines stated that Indeterminate cytology, reported as ‘‘follicular neoplasm’’ or ‘‘Hurthle cell neoplasm’’ can be found in 15–30% of FNA specimens and carries a 20–30% risk of malignancy, while lesions reported as atypia or follicular lesion of undetermined significance are variably reported and have a 5–10% risk of malignancy. While certain clinical features, such as male sex and nodule size (>4 cm) (66), older patient age, or cytologic features such as atypia, can improve the diagnostic accuracy for malignancy in patients with indeterminate cytology, overall predictive values remain low. Many molecular markers have been evaluated to improve diagnostic accuracy for indeterminate nodules. Many of these markers are available for commercial use in reference laboratories.
Each suspicious biopsy is sent for the molecular assessments for DNA-based markers and RNA-based markers (Afirma-Veracyte):
Afirma (Veracyte) - Gene Classifier
The Afirma Thyroid FNA Analysis combines specialized cytopathology and the novel Afirma Gene Expression Classifier (GEC). Physicians submit Veracyte thyroid nodule FNA samples collected in a single patient visit. Then, a thyroid cytopathology specialist at Thyroid Cytopathology Partners (TCP), an independent partner of Veracyte, performs a cytopathology assessment of a thyroid nodule FNA sample under the microscope. If the cytopathology diagnosis is benign or malignant, the analysis is complete. Only when TCP's cytopathology diagnosis is indeterminate (a recent study showed TCP’s indeterminate rate to be 16%) is the proprietary Gene Expression Classifier performed.


Afirma Test Kit

Afirma Chip for Gene Expression Classifier (GEC)

Sample of Afirma biopsy report
Thyroglobulin (TG) measurement on fine-needle washout fluids of LYMPH NODES BIOPSY
Thyroglobulin (Tg) measurement on fine-needle aspiration (FNA) specimens of neck lymph nodes is useful in the management of patients with papillary thyroid carcinoma when we suspect metastatic disease. The diagnosis of lymph node metastasis in patients with papillary thyroid cancer is an important factor when deciding to perform neck dissection at the initial surgery, as well as for evaluating the lymph node enlargement after the surgery.
FNA biopsy is performed with the single needle stick (25GA). The sample will then be placed into the vial and sent out to the laboratory. It takes about 10 business days to get the result.
Presence of thyroglobulin (TG) within the lymph node indicates metastatic disease.

Ultrasound view of the Neck Lymph Node with metastatic disease in a patient with Papillary Thyroid Carcinoma
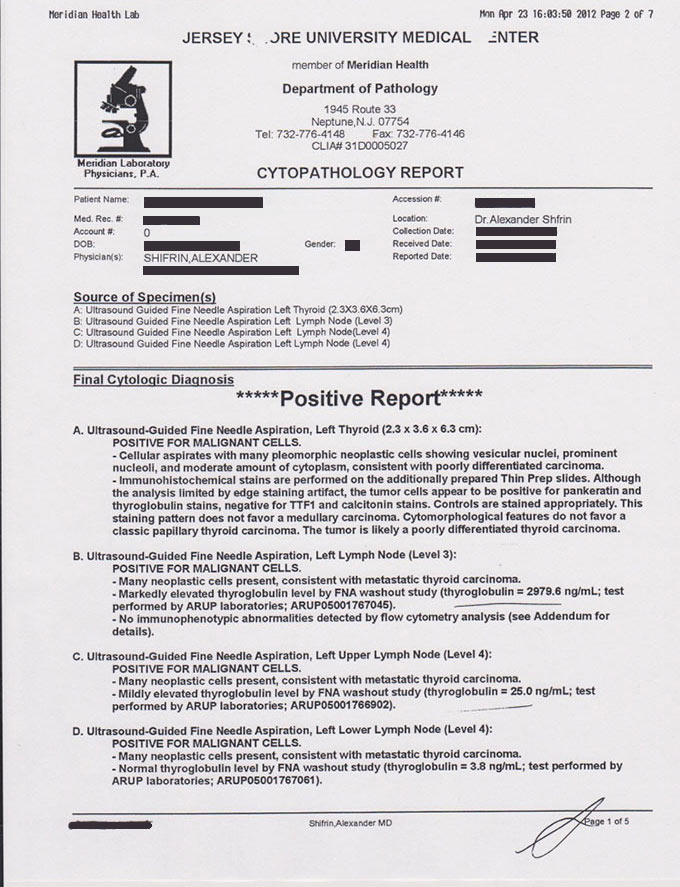
Example of the Report from Neck Lymph Node FNA biopsy in a patient with metastatic papillary thyroid carcinoma into the neck lymph nodes.
THYROID CYST ETHANOL ABLATION
If the thyroid nodule is completely cystic, then there is an option of percutaneous aspiration and ethanol injection (ablation) into the cyst. It is effective for managing predominantly cystic nodules and may require repeated injections. The procedure is performed under ultrasound guidance and is an outpatient procedure performed in the office. Not every patient with a cystic nodule would benefit. Only selected patients meet the criteria for ethanol ablation.


Before ethanol ablation



One year after ethanol ablation