Home
HomeThyroid Surgery
Minimally invasive thyroid surgery
1. Surgery for thyroid nodules and goiter (multinodular goiter)
2. Surgery for thyroid cancer
3. Surgery for Graves' disease
4. Surgery for toxic nodule goiter (toxic multinodular goiter or Plummer's disease)
5. Reoperative thyroid surgery
6. Neck lymph node dissections: central neck lymph dissection, modified radical neck dissection
7. Recurrent laryngeal nerve reconstruction
8. Surgery for familial endocrine syndromes: multiple endocrine neoplasia type 1 (MEN 1), MEN 2A and 2B syndromes
Minimally invasive thyroid surgery is the removal of one-half or the whole thyroid gland through a small mid-neck incision. The incision is placed in the natural skin crease. Minimally invasive thyroid surgery includes video-assisted or endoscopic thyroidectomy, when the surgeon uses a camera to magnify the view. This technique speeds up the healing process and results in minimal scar formation.
YOUR SURGERY:

Anesthesia
The procedure is done under general anesthesia. For some patients who can not tolerate or are not allowed to have general anesthesia (for example, during pregnancy), the procedure can be performed under local/regional anesthesia with general sedation. The latter one helps surgeons to use voice monitoring and avoid injury to important nerves that go to your vocal cords
Recurrent Laryngeal Nerve and External Branch of the Superior Laryngeal Nerve Monitoring during Thyroid Surgery
Recurrent Laryngeal Nerve Monitoring and External Branch of the Superior Laryngeal Nerve Monitoring are useful to identify the recurrent laryngeal nerve and/or External Branch of the Superior Laryngeal Nerve during Thyroid Surgery under general anesthesia. Monitoring is performed for all thyroid cases and parathyroid cases. A special endotracheal tube (ET) (breathing tube) with an electrode is used (picture below). The surgeon stimulates the nerve or, if it is difficult to find, the area where it is supposed to be. The signal is received by the ET tube and transmitted to the computer station at the back of the operating room. The technician will analyze visual and audio signals (see picture below). Nerve monitoring helps to identify and localize the nerve, to prevent complications such as injury to the nerve, it is also helps to identify the nerve and determine its function during cancer surgery, when cancer is growing over the nerve.

Endotracheal (ET) tube with the sensor for the recurrent laryngeal nerve monitoring during thyroid surgery.

Nerve monitoring during thyroid surgery, computer station.
Length of hospital stay
Surgery is performed as an outpatient procedure. The average stay after the surgery is about 6 hours. Most patients do not require an overnight stay. If the patient has significant comorbidities, or a very large goiter that extends into the chest cavity, or if the patient prefers to stay for social reasons, then the patient can stay overnight
Pain
Most patients have little or no pain. Some patients may feel discomfort or pressure after the surgery. Some patients may experience discomfort or pain while swallowing after surgery. It usually resolves within a couple of days. If the procedure is performed under local anesthesia with a nerve block, then some patients might feel shoulder/arm weakness after the neck block, which also resolves within 4-8 hours after the surgery
Postoperatively, most patients have no pain. If you do develop mild pain at home, you can take either Tylenol or Motrin.
Drain:
There will be NO drain placement.
Stitch and Scar:
The stitches will be removed the day of the surgery, right before you go home. You will have just a strip of skin glue on the skin. It will peel off on its own in about 6-10 days. Because the incision will be small and the stitch will be removed the same day of the procedure, the size of the scar will be much less than that of traditional thyroid surgeries performed in the past. The incision will be placed in the natural skin crease of your neck, which will help make it less noticeable or even invisible.
However, the tendency toward scarring depends on the individual's skin-healing properties. The surgeon will make every effort to achieve the best possible cosmetic result.
Complications:
Voice changes:
Only 1% (1 in 100 patients) experience complications related to the damage of the nerve that goes to the vocal cords. When this occurs, the patient will have a hoarse voice or an inability to make high-pitched sounds. More commonly, hoarseness lasts for a couple of days. In about 1 in 50 operations, patients may experience temporary changes in their voice, which resolve in 8 to 12 weeks.
Low calcium level:
In about 0.5% (1 in 200 operations) of total thyroid gland removal, the patient may experience low calcium levels. It occurs secondary to a malfunction of the parathyroid glands, which are located on or near the thyroid gland and share the same blood supply. If it happens, patients need to stay on calcium and vitamin D supplementation permanently. Because there are four parathyroid glands, this is rare. Because of the nature of the surgery, all patients with total thyroid removal will go home on calcium pills for 2-3 weeks. If the patient develops cramps in the hands or legs, or tingling in the face muscles, it indicates a low calcium level. In this case, you should immediately take 2 Calcium pills (1000 mg) and call your doctor.
For maximum absorption, Calcium should be supplemented with Magnesium.
Bleeding:
With the current technique, the bleeding rate is less than 0.5%.
Wound infection:
With the current technique, the incidence of wound infection is less than 0.5%. You do not need any antibiotics for the surgery, unless you have a condition that requires antibiotics with every procedure.
POSTOPERATIVE CARE:
Incision site:
The skin glue will peel off on its own in 6-10 days. After that, you can apply scar cream (usually silicone-based), Mederma, or lotion with Vitamin E 3-6 times a day to the wound. Try not to expose the wound to sunlight for about 1-2 months (especially during summer months), as this can cause skin discoloration in the wound area and make it look different from the surrounding skin.
Physical restrictions:
It is better not to drive for several days if you feel uncomfortable moving your neck. Do not drive if you are taking narcotics such as Percocet or Vicodin. There are no significant physical restrictions, but it is not advisable to perform any neck-stretching exercises for 2-3 weeks. Most patients resume their regular physical activities within a day of surgery.
Shower:
You can take a shower 2 days after the surgery. Do not scratch or peel off the skin glue; wipe it with the towel.
Pathology report:
Usually available within 5-7 days after the surgery
Problem calls:
Please call a doctor immediately if you develop significant neck swelling or shortness of breath shortly after surgery, or if you develop cramps in your hands or legs after surgery.
Postoperative visit:
2-3 weeks after the surgery: for wound check and pathology report.
Nurse Navigator:
For complex thyroid cancer-related postoperative care, we will assign the nurse navigator with expertise in taking care of thyroid cancer patients. Hurse navigator will help the patient coordinate care before and after surgery. She will also coordinate the Endocrine Cancer Tumor Board.
Wellness Protection Program: The Thyroid Cancer Survivor Story and Recovery Protocol by K. Napoli and A. Shifrin
Wellness Protection Program: The Thyroid Cancer Survivor Story and Recovery Protocol is awailable on Amazon, 215 pages, June 23, 2025, ISBN-13: 979-8288136207. Katie, a thyroid cancer survivor, shares her deeply personal journey of resilience, growth, and healing. Life’s unpredictable challenges have shaped her identity, and rather than fear these obstacles, she has chosen to embrace them. Her story is not only about battling cancer but about learning how to live fully after treatment—navigating survivorship with strength, purpose, and intention. With the guidance of Dr. Alexander Shifrin, Surgical Director of Endocrinology at Atlantic Health, CentraState Medical Center, Katie’s experience reveals a critical gap in traditional medical care: while physicians focus on diagnosis and active treatment, little structured support exists once the acute phase of care ends. Patients often face an uncertain path alone, needing guidance not only for physical recovery but also for emotional, mental, spiritual, and lifestyle healing. Recognizing this unmet need, Katie and Dr. Shifrin introduce the Wellness Protection Program—an integrative support system designed to accompany patients through every stage of survivorship. This protocol moves beyond conventional medicine, providing a comprehensive approach that includes nutritional guidance, lifestyle modification, mental health support, spiritual care, physical rehabilitation, and ongoing education. Rather than a one-time intervention, it is a lifelong framework to help survivors rebuild, maintain balance, and protect their long-term well-being. The Wellness Protection Program empowers thyroid cancer survivors to regain control over their health, offering structure, community, and hope long after active treatment ends.
POST-OPERATIVE SCAR GALLERY:
CLICK HERE TO SEE MORE IMAGES

Scar, 2 weeks after minimally invasive thyroid lobectomy surgery (1/2 of the thyroid removed)

Scar, 2 weeks after minimally invasive total thyroidectomy

Scar, 2 weeks after minimally invasive total thyroidectomy

Scar, 2 weeks after minimally invasive total thyroidectomy

Scar, 2 weeks after minimally invasive thyroid lobectomy (1/2 of the thyroid removed)

Patient with Graves' Disease. Scar 2 weeks after minimally invasive total thyroidectomy.

Scar 3 weeks after minimally invasive total thyroidectomy.

Scar 6 weeks after minimally invasive total thyroidectomy.

Scar 6 months after minimally invasive thyroid lobectomy (1/2 of the thyroid removed).

Scar, 2 years after minimally invasive thyroid lobectomy (1/2 of the thyroid removed)

Scar, 9 months after minimally invasive total thyroidectomy

Scar, 9 months after minimally invasive total thyroidectomy
 Scar. Patient with papillary thyroid carcinoma who has had the first surgery 5 weeks prior (1/2 of the thyroid was removed). Patient came back for completion of total thyroidectomy that included removal of the remaining ½ of the thyroid and lymph nodes in the central neck compartment (level 6 and 7), Second incision was placed in the old scar. This picture represents the second scar 2 weeks after the second surgery.
Scar. Patient with papillary thyroid carcinoma who has had the first surgery 5 weeks prior (1/2 of the thyroid was removed). Patient came back for completion of total thyroidectomy that included removal of the remaining ½ of the thyroid and lymph nodes in the central neck compartment (level 6 and 7), Second incision was placed in the old scar. This picture represents the second scar 2 weeks after the second surgery.

Scar, 1 year after thyroid lobectomy.
 Scar, 1.5 years after a total thyroidectomy for cancer.
Scar, 1.5 years after a total thyroidectomy for cancer.

Scar, 5 years after a total thyroidectomy for follicular thyroid carcinoma.
 Scar, 3 years after a total thyroidectomy with modified radical neck dissection (removal of entire right neck lymph nodes) on the right side for advanced thyroid cancer with metastatic disease to the right side neck lymph nodes
Scar, 3 years after a total thyroidectomy with modified radical neck dissection (removal of entire right neck lymph nodes) on the right side for advanced thyroid cancer with metastatic disease to the right side neck lymph nodes

Image on operating table, right after the completion of minimally invasive total thyroidectomy: you can see total thyroid with multiple nodules, above the thyroid is an incision which is closed with temporally placed stitch. The size of the incision is much smaller than the size of the thyroid with nodules.jpg

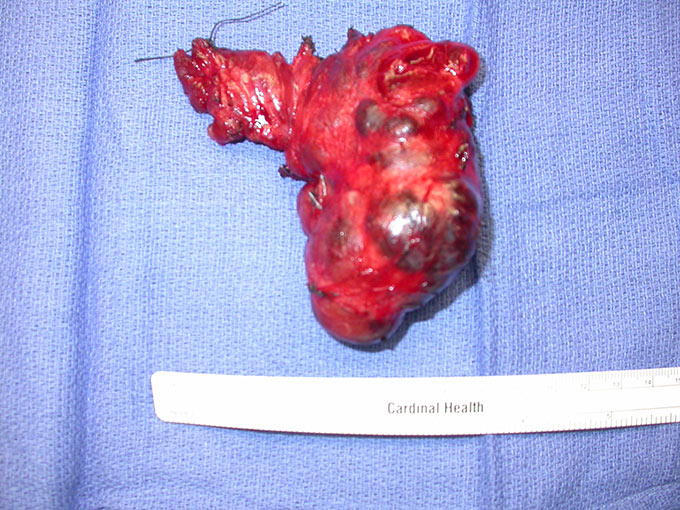
Total thyroid with cancer (papillary thyroid carcinoma) in the right thyroid lobe

Gigantic total thyroid gland extended into the chest cavity on the left side and resulted in airway compression.
 This picture represents a new scar within the old scar: patient is 2 weeks after completion of total thyroidectomy - removal of the remaining 1/2 (left side) of the thyroid after her prior surgery - removal of 1/2 of the thyroid (right side) that was done with a big scar 30 years ago (the new scar is much smaller, was placed into the old scar and it is invisible within the old scar)
This picture represents a new scar within the old scar: patient is 2 weeks after completion of total thyroidectomy - removal of the remaining 1/2 (left side) of the thyroid after her prior surgery - removal of 1/2 of the thyroid (right side) that was done with a big scar 30 years ago (the new scar is much smaller, was placed into the old scar and it is invisible within the old scar)

Scar, 2 weeks after a total thyroidectomy with central neck lymph nodes dissection (lymph nodes removal from the central neck) for Papillary Thyroid Carcinoma

Scar, 2 weeks after the left thyroid lobectomy (left 1/2 of the thyroid removed)

Scar, 3 months after total thyroidectomy
 Scar, 2 weeks after the left thyroid lobectomy (left 1/2 of the thyroid removed) as a completion of total thyroidectomy for papillary thyroid carcinoma. First surgery was 4 weeks prior, only the final pathological report has revealed cancer in the right side nodule, andthe patient had to go back for a completion of total thyroidectomy (new incision was placed in the old scar)
Scar, 2 weeks after the left thyroid lobectomy (left 1/2 of the thyroid removed) as a completion of total thyroidectomy for papillary thyroid carcinoma. First surgery was 4 weeks prior, only the final pathological report has revealed cancer in the right side nodule, andthe patient had to go back for a completion of total thyroidectomy (new incision was placed in the old scar)

Left Thyroid lobe with a large, 4 cm, nodule (Follicular Neoplasm by preoperative FNA Biopsy)

Scar, 2 weeks after the right thyroid lobectomy (removal of the right 1/2 of the thyroid) for 6 cm (2 and 1/4 inches) hyperfunctioning nodule.

Scar, 2 weeks after a total thyroidectomy with central neck (level 6 and 7) lymph nodes dissection for metastasis to the lymph nodes Papillary Thyroid Carcinoma.

Scar, 2 weeks after total thyroidectomy for small Papillary Thyroid Carcinoma.

Scar, 2 weeks after the right thyroid lobectomy (removal of the right 1/2 of the thyroid) for a 2.6 cm (about 1 inch) thyroid nodule.

Scar, 2 weeks after the left thyroid lobectomy (removal of the left 1/2 of the thyroid) for a 3.1 cm (about 1 inch and 1/2) Follicular Adenoma.

A large thyroid goiter with multiple nodules that has extended inside the chest cavity on the left side (multinodular goiter measured 3 and 1/2 inches in width with intrathoracic extension on the left).

Scar, 2 weeks after a total thyroidectomy in a patient with goiter, as shown in the picture above: no chest split was performed, and the entire procedure was performed through the neck; this scar is less than 2 inches, while the thyroid goiter itself measures 3 and 1/2 inches.

A large multinodular thyroid gland with extension of the entire right side into the right chest cavity. Surgery was performed through the neck incision without chest opening.

Scar, 2 weeks after a total thyroidectomy for a small Papillary Thyroid Carcinoma.

Scar, 1 year and 3 months after a total thyroidectomy with central neck (level 6 and 7) lymph nodes dissection for a Papillary Thyroid Carcinoma.

Scar, 2 weeks after the right thyroid lobectomy (removal of the right side of the thyroid gland) for follicular adenoma that was measuring 4.5 x 2.1 x 3.1 cm (almost 2 inches in size), the scar is less than 2 inches

Scar, 2 weeks after a total thyroidectomy for a small Papillary Thyroid Carcinoma (multifocal micropapillary thyroid carcinoma) in one lobe and a follicular adenoma in another lobe.

Scar, 2 weeks after a total thyroidectomy.

Scar, 2 weeks after a total thyroidectomy for multinodular goiter.

Scar, 2 weeks after a total thyroidectomy with central neck lymph nodes (level 6 and 7) dissection for papillary thyroid carcinoma.

Scar, 2 weeks after a total thyroidectomy for a 2.1 cm (about an inch) Papillary Thyroid Carcinoma on the right side.
Gigantic thyroid gland that was removed in a 42-year-old female (picture below). The gland was extending inside her left chest cavity for about 4 -5 inches. It was almost completely inside of her left chest cavity, and was not noticeable on the direct neck examination, but could only be seen on the CT scan. It was completely removed through the neck incision without splitting her chest bone (sternum)

Scar, 2 weeks after a total thyroidectomy in the patient mentioned above. The patient had only a neck incision for the removal of this gigantic thyroid gland that had extended inside her chest cavity for about 4 -5 inches on the left. It was completely removed through the neck incision without splitting her chest bone (sternum)

Scar, 3 months after a total thyroidectomy for Follicular Thyroid Carcinoma in a 73-year-old male patient. The patient also had radioactive iodine treatment after the surgery

Scar, 2 weeks after a total thyroidectomy with central neck lymph nodes (level 6 and 7) dissection for papillary thyroid carcinoma in a 22-year-old female.

Scar, 7 years after total thyroidectomy for Graves' disease.

Scar, 2 weeks after the total thyroidectomy for papillary thyroid carcinomas 3 cm and 3.2 cm in the right thyroid lobe.

Scar, 2 weeks after a total thyroidectomy with central neck lymph nodes (level 6 and 7) dissection for a 2.5 cm (1 inch) papillary thyroid carcinoma in a 22-year-old female.

Scar, 3 years after a left thyroid lobectomy in 25-year-old female for 2 cm x 2 cm (less than an inch) follicular adenoma.