Home
HomePrimary Hyperparathyroidism
Primary Hyperparathyroidism
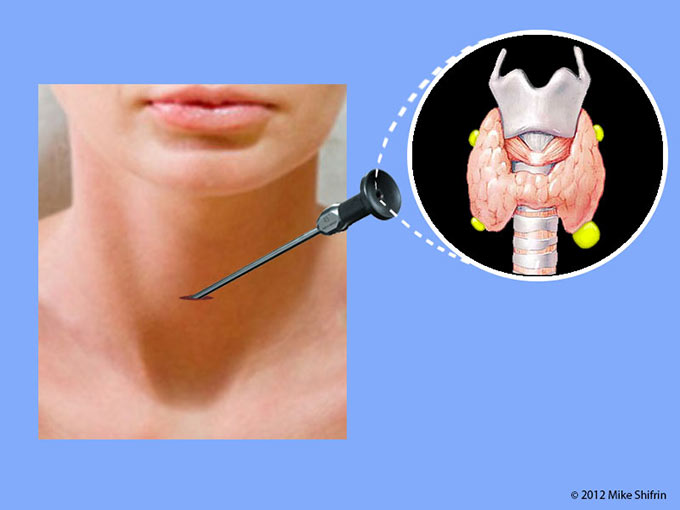
Parathyroid glands

There are four parathyroid glands in our body. They are very small, about 1/5 of an inch, and located on or behind the thyroid gland in the neck, or elsewhere in this area: usually two on the top and two on the bottom on each side of the neck. Parathyroid glands have sensors that detect the amount of calcium in the bloodstream. They function normally to regulate calcium and phosphorus levels by secreting parathyroid hormone (PTH). PTH regulates the level of calcium in the blood, the release of calcium from bone, the absorption of calcium in the intestine, and the excretion of calcium in the urine. When blood calcium levels fall, the parathyroid glands secrete PTH to stimulate calcium reabsorption in the kidneys and to release calcium from bone.
What is hyperparathyroidism?
Calcium plays an important role in bone development and in maintaining bone strength. Calcium is also important in nerve transmission and muscle contraction. Hyperparathyroidism is a disorder of the parathyroid glands characterized by hyperfunctioning, or excessive secretion, of parathyroid hormone (PTH). Primary hyperparathyroidism is a disorder of one (in 85% of the patients) or more than one (in 15% of the patients) parathyroid gland. This problem originates in the parathyroid glands, in contrast to secondary or tertiary hyperparathyroidism, which causes the parathyroids to be overactive secondary to conditions such as kidney failure.
What is primary hyperparathyroidism?
When the parathyroid gland (or glands) becomes hyperfunctional and enlarged, it ignores our body's needs. It secretes excess parathyroid hormone (PTH) into the bloodstream, raising calcium levels. The normal feedback mechanism that prevents PTH overproduction is disrupted, and one (or several) of the parathyroid glands loses its calcium-sensing ability and starts functioning independently of the body's needs. Excessive accumulation of calcium in the blood is called hypercalcemia. A parathyroid adenoma, a benign, overactive tumor of the parathyroid gland, usually causes Primary Hyperparathyroidism. Enlargements of all four glands are called multiglandular parathyroid disease or hyperplasia. In 85 percent of people with primary hyperparathyroidism, there is only one adenoma, and in 15 % of people, there may be more than one adenoma or hyperplasia. Rarely, less than 1 % of people may have cancer of the parathyroid gland.
This excess PTH release into the bloodstream may pull calcium out of the bones and cause osteopenia and then osteoporosis. Osteoporosis may then result in bone fractures. Calcium levels may increase in the urine, leading to kidney stones. PTH also lowers blood phosphorus levels by increasing urinary phosphorus excretion. Excess of calcium in the bloodstream may also result in excessive deposition of calcium in other parts of our body, including vessels.
The vast majority of primary hyperparathyroidism is idiopathic. It means that we do not know the reason for that. Sometimes it is linked to exposure to radiation. In about 5 percent of cases, the condition can be linked to an inherited condition—syndrome. Familial multiple endocrine neoplasia type 1 (MEN 1) syndrome is a rare, inherited syndrome that affects the parathyroids as well as the pancreas and the pituitary gland. Familial multiple endocrine neoplasia type 2 A (MEN 2A) syndrome also affects the thyroid gland (medullary thyroid carcinoma) and the adrenal gland (pheochromocytoma). It is important to rule out familial hypocalciuric hypercalcemia (FHH) syndrome because this syndrome does not require treatment. This is why it is important to be evaluated by a specialist (an endocrinologist or endocrine surgeon) who is familiar with this syndrome and can determine whether further testing is needed.
How common is hyperparathyroidism?
In the United States, about 100,000 people develop the disorder each year. It is the third most prevalent endocrine disease, following diabetes mellitus and thyroid disorders. Women outnumber men two to one, and risk increases with age, occurring in 1/500 females and 1/2,000 males over the age of 40. In women 60 years and older, two out of 1,000 will develop hyperparathyroidism each year. A history of childhood irradiation to the face or neck is a risk factor for the development of primary hyperparathyroidism. Primary hyperparathyroidism is a more common disorder than previously documented. It is crucial to evaluate even mild hypercalcemia because 43% of these patients have primary hyperparathyroidism. Primary hyperparathyroidism is underdiagnosed and undertreated.
What are the symptoms of primary hyperparathyroidism?
Most commonly, the patient had no symptoms and she or he was found to have an elevated blood calcium level on a routine blood test.
When symptoms do appear, they are often mild and nonspecific, such as a feeling of weakness, tiredness, fatigue, depression, memory problems, muscle aches and bone pains, constipation, frequent urination, sleep disturbance, and anxiety.
With more severe disease, increased calcium excretion in the urine may cause kidney stones. The most common complication of primary hyperparathyroidism is kidney stones, with an incidence of 15% to 20%. Other renal manifestations of primary hyperparathyroidism include hypercalciuria, which is seen in approximately 40% of affected patients. An unexplained reduction in creatinine clearance has also been regarded as a potential renal complication of primary hyperparathyroidism. Increased bone resorption can lead to fractures in situations where they would not normally occur. A person may have a loss of appetite, nausea, vomiting, severe constipation, impaired thinking, memory, and confusion. In more severe cases, the disease progresses to the point of psychosis, which would result in admission to the hospital, and in the most extreme cases, "hypercalcemic crisis" may develop, and the patient may become comatose. It has been recently reported that up to 30% of patients with Primary Hyperparathyroidism actually have significant symptoms of depression, and one third of those 30% are reported to have suicidal ideas. Sleep impairment is prevalent in patients with primary hyperparathyroidism, with a reported incidence of 44 %.
How to make a diagnosis of primary hyperparathyroidism?
Hyperparathyroidism is diagnosed by checking blood calcium and PTH levels and finding that both of them are elevated. Other diseases can cause elevated calcium levels and have to be ruled out as well, but only hyperparathyroidism results in elevated calcium and parathyroid hormone levels. When the PTH level is not above the upper normal limit, it tends to be in the upper range of normal; however, in the setting of hypercalcemia, even a normal value is not normal. Another variant of primary hyperparathyroidism has been described in which the total and ionized serum calcium are consistently normal, but the PTH level is persistently elevated. This is called normocalcemic primary hyperparathyroidism. To diagnose normocalcemic primary hyperparathyroidism, all causes for a secondary hyperparathyroid state must be considered and excluded (for example, vitamin D insufficiency).
Once the diagnosis is established, other tests may be done to localize the disease, such as one gland versus several glands.
Because high PTH levels can cause bone loss, a measurement of bone density can help assess bone loss and the risk of fractures. An abdominal ultrasound may reveal kidney stones. A 24-hour urine collection for calcium needs to be performed to rule out familial hypocalciuric hypercalcemia (FHH) and provide information on increased urinary calcium excretion by the kidneys.
How is primary hyperparathyroidism being treated?
The newest Guidelines, "The Surgical Management of Asymptomatic Primary Hyperparathyroidism: Proceedings of the Fourth and Fifth International Workshop," indicated that all patients with Primary Hyperparathyroidism who meet surgical criteria should be referred to an experienced endocrine surgeon to discuss the risks, benefits, and potential complications of surgery. Patients who do not meet surgical criteria and have no medical contraindications to surgery may request a visit with an experienced endocrine surgeon. Alternatively, a multidisciplinary endocrine conference with surgeon involvement could be employed to address all relevant issues. 3) Imaging is not a diagnostic procedure; it is a localization procedure to help the surgeon optimize the operative plan. 4) The frequency of hereditary forms of Primary Hyperparathyroidism may be underappreciated and needs to be assessed with increased vigilance. And 5) surgery is likely to benefit patients due to high cure rates, low complication rates, and the likelihood of reversing skeletal manifestations.
Past Guidelines for the Management of Asymptomatic Primary Hyperparathyroidism: Summary Statement from the Third International Workshop guided the use of diagnostics and management for this condition in clinical practice.
The best treatment option for a patient with Primary Hyperparathyroidism (those who meet surgical criteria) is minimally invasive parathyroidectomy. Your surgeon should have expertise in parathyroid surgery and perform at least 50 to 100 parathyroidectomies per year to be considered an expert. To perform minimally invasive parathyroid surgery, the surgeon will need high-quality parathyroid localization studies, including a Sestamibi scan (and, if possible, Spect CT Sestamibi, which has much higher sensitivity than Sestamibi alone) and a designated neck/parathyroid ultrasound, and a 4D CT scan. Intraoperative PTH monitoring is the key to success. It helps surgeons achieve surgical cure with intraoperative confirmation of a drop in PTH level to normal ranges; a more than 50% drop in PTH level from pre-excision to 10 minutes post-excision is considered a surgical success (per Miami criteria by Dr. Irving).
All patients with biochemically confirmed primary hyperparathyroidism who have specific symptoms of their disease, such as kidney stones, fractures, or severe psychosis as a result of "hypercalcemic crisis," should undergo surgical treatment. Because surgery is always considered the definitive therapy for this disease, even in asymptomatic subjects, a decision to elect medical monitoring should follow guidelines based on the severity of the disease's manifestations, and patients should be appropriately monitored. New data on the natural history of asymptomatic primary hyperparathyroidism have favored surgery because bone density does not appear to be indefinitely stable. Moreover, up to one-third of patients who are monitored long-term develop signs of disease progression. It has also been demonstrated that bone density increases consistently after parathyroidectomy, accompanied by decreases in bone turnover.
Guidelines for surgery (which patient needs surgery)
Surgical management is often indicated for primary hyperparathyroidism (PHPT) based on specific clinical indications and guidelines. Primary hyperparathyroidism is a condition characterized by overactivity of the parathyroid glands, leading to elevated levels of parathyroid hormone (PTH) and calcium in the blood. Surgical intervention is the definitive treatment for most cases of primary hyperparathyroidism.
Guidelines for Surgery in Asymptomatic Primary Hyperparathyroidism:
Serum Calcium 1.0 mg/dL (0.25 mmol/L) above the upper limit of normal
Skeletal disease - bone mineral density (BMD by DEXA) T-score < -2.5 at lumbosacral spine, BMD by DXA: T-score < 2.5 at total hip, femoral neck, or distal1/3 radius.Vertebral fracture by X-ray, CT, MRI, or VFA
Kidney disease - eGFR <60 cc/min, Complete 24-hour urine for calcium>250 mg/day in women(>6.25 mmol/day) or> 300 mg/day in men(>7.5 mmol/day)c. Presence of nephrolithiasis or nephrocalcinosis by X-ray, ultrasound, or CT
Age <50 years
Surgery for primary hyperparathyroidism typically involves the removal of the abnormal parathyroid gland(s). This can be done through various surgical approaches, including minimally invasive parathyroidectomy or traditional bilateral neck exploration.
Individuals with primary hyperparathyroidism need to discuss their specific case with a healthcare professional, typically an endocrinologist or a surgeon, to determine the most appropriate course of action based on their clinical presentation and overall health. Treatment decisions are often made on a case-by-case basis, and guidelines may evolve, so it's crucial to consult with healthcare providers for the latest recommendations.
Surgery to remove the enlarged parathyroid gland (or glands) is curative in 95 percent of patients. The best approach is to perform a minimally invasive parathyroidectomy. to have procedure as a minimally invasive surgery, good preoperative localization with parathyroid ultrasound and Sestamibi scan, as well as an intra-operative PTH monitoring are essential.
Medical Management of Primary Hyperparathyroidism: Proceedings of the Fourth International Workshop on the Management of Asymptomatic Primary Hyperparathyroidism.
Patients with low serum 25-hydroxyvitamin D should be repleted with vitamin D doses aiming to raise serum 25-hydroxyvitamin D levels to ≥50 nmol/L, with a goal of ≥75 nmol/L (30 ng/mL). Medications should be reserved for patients in whom lowering serum calcium and/or increasing bone mineral density is desirable. For the control of hypercalcemia, cinacalcet (Sensipar) is the treatment of choice. Cinacalcet reduces serum calcium concentrations to normal ranges, but has almost no effect on serum PTH levels. However, bone mineral density does not change!!!. To improve bone mineral density, bisphosphonate therapy, such as alendronate, is recommended. Alendronate improves bone mineral density at the lumbar spine without altering serum calcium concentration. To reduce serum calcium and improve bone mineral density, combination therapy with both agents is reasonable, but strong evidence for its efficacy is lacking. Per manufacturer indication on Sensipar Label: "1.3 Primary Hyperparathyroidism Sensipar is indicated for the treatment of hypercalcemia in adult patients with primary HPT for whom parathyroidectomy would be indicated based on serum calcium levels, but who are unable to undergo parathyroidectomy
Conservative medical therapy, such as use of calcimimetics (Sensipar), a new class of drug that "turns off" secretion of PTH, without lowing PTH level. This group of medications has been approved by the Food and Drug Administration only for the treatment of hyperparathyroidism secondary to kidney failure with dialysis (secondary hyperparathyroidism), and persistent primary hyperparathyroidism caused by parathyroid cancer that failed surgery or reoccurred as a metastatic disease .
Some patients who have mild disease, do not have surgical indications, and do not need immediate treatment, long-term monitoring is performed. Periodic monitoring would include clinical evaluation, measurement of serum calcium and PTH levels, evaluation for kidney stones, and bone mass measurement. If the patient or physician chooses long-term follow-up, the patient should try to drink lots of water, get plenty of exercise, and avoid certain diuretics, such as the thiazides. Immobilization (inability to move) and gastrointestinal illness, including vomiting or diarrhea, can raise calcium levels. Patients with hyperparathyroidism should seek medical attention if they find themselves immobilized, vomiting, or having diarrhea.

Parathyroid adenoma

Parathyroid adenoma

Hyperplastic parathyroid gland under high magnification microscope
Advantages of minimally invasive parathyroidectomy
Less pain
Less requirement for analgesia
Less consumption of analgesics
Less scarring
Less hospital stays
Greater cosmetic satisfaction
Faster recovery
Prognosis
After parathyroid surgery, serum and urinary calcium levels and the serum PTH level return to normal. After successful parathyroid surgery, increases in bone mineral density (decreasing the risk of fractures and improving osteoporosis) are observed at the lumbar spine and hip regions, and, after a delay, at the distal one-third of the radius as well. Bone mineral density increases after parathyroid surgery by approximately 10% to 12% at the lumbar spine and hip. Fracture-free survival is significantly improved with surgery compared with no surgery. Increases at the lumbar spine, hip, and distal radius are sustained over 10 to 15 years after surgery.
Almost half of the postmenopausal women with hyperparathyroidism and low bone mineral density have a significant remineralization (bone recovery) response 1 year after parathyroidectomy. Those patients who gain the most bone mineral density recovery are younger, have more severe hyperparathyroidism, and have better renal function before surgery.
In patients who underwent parathyroid surgery because of their renal stone disease, there were no recurrences of nephrolithiasis over a decade. Parathyroidectomy results in improvement of some neuropsychiatric parameters, such as cognition, mood, anxiety, and memory.
Recent data indicated that the recurrence rate after parathyroidectomy is between 2.1% and 2.5% regardless of the type of surgery, either open parathyroidectomy or minimally invasive parathyroidectomy. The percentage decrease in intraoperative PTH was protective against recurrence for both approaches. A higher postoperative PTH also independently predicted disease recurrence.
Timing of symptom improvement after parathyroidectomy for primary hyperparathyroidism:
Symptom improvement was most pronounced 6 weeks post-parathyroidectomy, although some symptoms continued to improve at 6 months. Fatigue and bone/joint pain demonstrated "Immediate Improvement" (>50% of patients reporting improvement by post-operative week 1), whereas the majority of symptoms showed peak improvement at 6 weeks ("Delayed Improvement"). Symptoms categorized as "Continuous Improvement" were those showing progressive improvement up to 6 months postoperatively (polydipsia, headaches, and nausea/vomiting).
Are there any complications associated with parathyroid surgery?
Surgery for hyperparathyroidism is highly successful with a low complication rate when performed by surgeons experienced with this condition. About 1 percent of patients undergoing surgery experience damage to the recurrent laryngeal nerve, which controls the vocal cords' function; this can affect speech and result in hoarseness. One percent of patients lose all their parathyroid tissue and thus develop chronic low calcium levels (hypoparathyroidism), which may require treatment with multiple doses of calcium with vitamin D a day. The complication rate is slightly higher for hyperplasia than it is for adenoma since more extensive surgery is needed. The complication rate depends on the surgeon's experience performing these procedures.
What happens if parathyroid surgery is not performed for primary hyperparathyroidism?
Most patients with mild, asymptomatic primary hyperparathyroidism who have been followed up for up to 15 years without surgery or specific medical therapy have stable calcium and PTH levels for the first 10 years. Serum calcium, however, does tend to increase slightly during years 10 to 15. For the first 10 years, bone mineral density is stable, but over the next 5 years, declines are seen at the hip and the one-third distal radius. Thirty-seven percent of patients followed up for up to 15 years met one or more indications for parathyroid surgery.
Are parathyroid imaging studies needed before surgery?
To perform minimally invasive parathyroid surgery, the two most commonly used localization tests are performed before surgery to find the parathyroid adenoma. Those two tests are: neck parathyroid ultrasound and Sestamibi (parathyroid) scan. .
Patients with primary hyperparathyroidism who do not have Sestamibi and ultrasound imaging showing a parathyroid adenoma are at higher risk of persistent disease. Staudy have shown that in patients who had undergone dual imaging with an ultrasound scan and sestamibi scintigraphy, failure rates with surgery was 2% if both imaging have shown the same site of the adenoma (with specific indication on the upper or lower gland), 9% - if both imagining only have agreed on the side (without specific indication on the upper or lower gland), and 11% - if both imaging are negative for findings of the adenoma.

Sestamibi Scan showing right lower parathyroid adenoma


Neck Ultrasound showing parathyroid adenoma
Click on image to view video “Minimally Invasive Video-Assisted Parathyroidectomy
Familial Primary Hyperparathyroidism
- Familial isolated primary hyperparathyroidism (FIHP) is a rare hereditary disorder characterized by hypercalcemia, high parathyroid hormone (PTH) level, and isolated parathyroid tumors. FIHP was suggested as being a syndrome clinically and genetically distinct from multiple endocrine neoplasia (MEN), familial hypocalciuric hypercalcemia, and hyperparathyroidism-jaw tumor syndrome. No specific genetic anomaly has been reported in FIHP
- Five genetic syndromes are associated with Familial Primary Hyperparathyroidism and result from specific gene mutations, such as the multiple endocrine neoplasia type 1 (MEN1), multiple endocrine neoplasia type 2A (MEN2A), MEN type 4, MEN type 5, and hyperparathyroidism-jaw tumor (HPT-JT) syndromes.
Familial Primary Hyperparathyroidism has a younger age at diagnosis and an equal development between affected men and women.
References:
Bilezikian JP, Khan AA, Potts JT Jr; Third International Workshop on the Management of Asymptomatic Primary Hyperthyroidism. J Clin Endocrinol Metab. 2009 Feb;94(2):335-9.
The diagnosis and management of asymptomatic primary hyperparathyroidism revisited.
Khan AA, Bilezikian JP, Potts JT Jr; Guest Editors for the Third International Workshop on Asymptomatic Primary Hyperparathyroidism.
Sara Murray, Priya Pathak, Sarah Schaefer, Herbert Chen. Rebecca Sippel. Improvement of Sleep Disturbance and Insomnia Following Parathyroidectomy for Primary Hyperparathyroidism. World J Surg (2014) 38:542–548
Presentation of asymptomatic primary hyperparathyroidism: proceedings of the third international workshop. Silverberg SJ, Lewiecki EM, Mosekilde L, Peacock M, Rubin MR. J Clin Endocrinol Metab. 2009 Feb;94(2):351-65.
Diagnosis of asymptomatic primary hyperparathyroidism: proceedings of the third international workshop. Eastell R, Arnold A, Brandi ML, Brown EM, D'Amour P, Hanley DA, Rao DS, Rubin MR, Goltzman D, Silverberg SJ, Marx SJ, Peacock M, Mosekilde L, Bouillon R, Lewiecki EM. J Clin Endocrinol Metab. 2009 Feb;94(2):340-50.
Ann Surg. 2013 Nov 20. Predictors of Recurrence in Primary Hyperparathyroidism: An Analysis of 1386 Cases. Schneider DF, Mazeh H, Chen H, Sippel RS.
John P. Bilezikian, Primary hyperparathyroidism. Endocr Pract. 2012;18:781-790
A. Bagul, H. P. Patel, D. Chadwick, B. J. Harrison, S. P. Balasubramanian. Primary Hyperparathyroidism: An Analysis of Failure
of Parathyroidectomy. World J Surg (2014) 38:534–541
Bandeira F, Griz L, Chaves N, Carvalho NC, Borges LM, Lazaretti-Castro M, Borba V, de Castro LC, Borges JL, Bilezikian J. Diagnosis and management of primary hyperparathyroidism--a scientific statement from the Department of Bone Metabolism, the Brazilian Society for Endocrinology and Metabolism. Arq Bras Endocrinol Metabol. 2013 Aug;57(6):406-24.
Cipriani C, Romagnoli E, Cilli M, Piemonte S, Pepe J, Minisola S. Quality of life in patients with primary hyperparathyroidism. Expert Rev Pharmacoecon Outcomes Res. 2014 Feb;14(1):113-21.
Press DM, Siperstein AE, Berber E, Shin JJ, Metzger R, Monteiro R, Mino J, Swagel W, Mitchell JC. The prevalence of undiagnosed and unrecognized primary hyperparathyroidism: a population-based analysis from the electronic medical record. Surgery. 2013 Dec;154(6):1232-7; discussion 1237-8.
Murray SE, Pathak PR, Pontes DS, Schneider DF, Schaefer SC, Chen H, Sippel RS. Timing of symptom improvement after parathyroidectomy for primary hyperparathyroidism. Surgery. 2013 Dec;154(6):1463-9.
Sitges-Serra A1, García L, Prieto R, Peña MJ, Nogués X, Sancho JJ. Effect of parathyroidectomy for primary hyperparathyroidism on bone mineral density in postmenopausal women. Br J Surg. 2010 Jul;97(7):1013-9.
Udelsman R1, Akerström G, Biagini C, Duh QY, Miccoli P, Niederle B, Tonelli F. The Surgical Management of Asymptomatic Primary Hyperparathyroidism: Proceedings of the Fourth International Workshop. J Clin Endocrinol Metab. 2014 Aug 27
Marcocci C1, Bollerslev J, Khan AA, Shoback DM. Medical Management of Primary Hyperparathyroidism: Proceedings of the Fourth International Workshop on the Management of Asymptomatic Primary Hyperparathyroidism. J Clin Endocrinol Metab. 2014 Aug 27
Silverberg SJ, Clarke BL, Peacock M, Bandeira F, Boutroy S, Cusano NE, Dempster D, Lewiecki EM, Jian-Min L, Minisola S, Rejnmark L, Silva BC, Walker MD, Bilezikian JP. Current Issues in the Presentation of Asymptomatic Primary Hyperparathyroidism: Proceedings of the Fourth International Workshop. J Clin Endocrinol Metab. 2014 Aug 27
Eastell R, Brandi ML, Costa AG, D'Amour P, Shoback DM, Thakker RV. Diagnosis of Asymptomatic Primary Hyperparathyroidism: Proceedings of the Fourth International Workshop. J Clin Endocrinol Metab. 2014 Aug 27
Bilezikian JP, Brandi ML, Eastell R, Silverberg SJ, Udelsman R, Marcocci C, Potts JT Jr. Guidelines for the Management of Asymptomatic Primary Hyperparathyroidism: Summary Statement from the Fourth International Workshop. J Clin Endocrinol Metab. 2014 Aug 27